
Change of the mental abilities is a normal process which affects the population already over 40 and even strengthens with age.



The proposal (excerpts)
Section 1: Objectives
Europe is ageing. The percentage of the population that is 65 year old or older as well as their life expectancy is rising. The number of elderly people will be more than doubled by 2050 and the proportion of people living alone will increase. The well-being of elderly citizens at home, at work and in the social life has a clear European dimension of high relevance (Recommendation 1796 (2007) of the Parliamentary Assembly of the European Council).
The change of mental abilities is a normal process which already affects the population over 40 and strengthens with the age. People over 65 and especially over 80 are typically more seriously affected. To recognize if and when normal deterioration turns into mental disorder is not easy for the specialists (psychiatrists or psychologists), and even less for the relatives and friends.
Reading books, playing card and board games, solving crosswords and other puzzles are popular tools for keeping the mind fresh. With the spread of computers and computer networks computerized games are becoming more and more popular among the elderly. There are many websites offering games for everyone, however, only few of them are designed for the elderly as far as content, ergonomics, psychology, abilities, etc. are concerned. On the other hand, a continuously increasing number of websites are opened for the 50+, 60+ and older which rarely offer on-line games for the visitors. Finally, there are also many websites addressing mental hygiene, mental freshness, mental disorders but they rarely build communities, offer computerized games or multinational co-operation.
A striking difference between traditional games and their computerized variants is the – rarely utilized – fact that the latter are also able to collect behavioural data in order to measure mental (and motoric) abilities and especially their changes over time. While this is a double-bladed possibility which raises several fundamental ethical and legal issues, no one can deny that “measuring is knowing”, that is, if we can measure states and especially state changes in a scientifically sound way and a strictly controlled environment then we can provide better and more timely help for the elderly and their families than without measurements and data processing.
The main objective of the project is to develop a mental wellness toolset for self usage (i.e. for the individuals and their families), and only to a lesser extent for the medical experts (psychiatrists, psychologists, carers, etc.) Our goal is to measure and visualize mental changes, tendencies in an entertaining way, and to give indications, sort of warnings, alarms or reports, to the effected persons and their relatives or friends that it is advisable to visit a physician. Our ambition is to compare one's mental wellness to his/her own past mental wellness conditions (in relative values), while it is definitely not our aim to compare one's mental ability to others' (in absolute values, like the Intelligence Quotient).
The major tasks in the planned project are the following:
- Develop a series of well-chosen on-line games, including community games, tailored for various kinds of elderly people that facilitate also the collection of measurement data related to their mental – and to some extent motoric – conditions and abilities.
- Develop a scientifically sound methodology for mental wellness measurement and data evaluation, which is also prepared for the clinical validation of this methodology.
- Develop an entertaining mental wellness toolset for self-use, based on the above results, tailored to provide maintenance and measurement facilities for elderly people's mental – and to some extent motoric – conditions and abilities with the goal to detect changes and tendencies.
- Build a multinational / multicultural mental wellness community (from groups already existing or to be formed in the countries participating in the planned project), backed with a multilingual website.
- Create multilingual content for the mental-wellness multinational / multicultural community, including on-line community games, consultancy services, on-line forums, etc.
1.1 Progress beyond the state-of-the-art and contribution to the knowledge in the field
Psychiatric assessment typically involves a mental status examination and the taking of a case history; neuropsychological and psychological tests may be also conducted.
Neuropsychological tests are specifically designed tasks used to measure a psychological function known to be linked to a particular brain structure or pathway. They usually involve the systematic administration of clearly defined procedures in a formal environment (single person, quiet office, no distractions). As such, it can be argued that neuropsychological tests at times offer an estimate of a person's peak level of cognitive performance. Neuropsychological tests are a core component of the process of conducting neuropsychological assessment.
Most neuropsychological tests in current use are based on traditional psychometric theory. In this model, a person's raw score on a test is compared to a large general population normative sample that should ideally be drawn from a comparable population. Normative studies frequently provide data stratified by age, level of education, and/or ethnicity, where such factors have been shown by research to affect performance on a particular test. This allows for a person's performance to be compared to a suitable control group, and thus provide a fair assessment of their current cognitive functioning.
Psychological testing is a field characterized by the use of samples of behaviour in order to infer generalizations about a given individual. The technical term for the science behind psychological testing is psychometrics. By samples of behaviour, one means observations over time of an individual performing tasks that have usually been prescribed beforehand, which often means scores on a test. These responses are often compiled into statistical tables that allow the evaluator to compare the behaviour of the individual being tested to the responses of a norm group. Psychological assessment is similar to psychological testing but usually involves a more comprehensive assessment of the individual. Psychological assessment is a process that involves the integration of information from multiple sources, such as tests of normal and abnormal personality, tests of ability or intelligence, tests of interests or attitudes, as well as information from personal interviews.
It can be concluded that the observation of changes in one’s mental abilities over time needs regular measurements, recording of the measured data, and evaluation and proper visualization of such historic data. Current methods are mostly used as clinical tests conducted by professionals under controlled environments, and cannot be used alone or in family circle in the home environment.
Our assumption is that entertaining on-line computer games can be developed for the purpose of measuring the changes of mental wellness, based on time series of properly chosen data. Such a game can either realize one of the well-proven standard tests, or combine some of the proven tests in an interesting and entertaining story. The R&D challenge is to find the proper balance between validated tests and entertaining solution. Our second assumption is that the detection of changes in one’s mental wellness is significantly easier to accomplish than to measure mental abilities in “absolute” values, i.e. in comparison to specific averages or norms. We even believe that change detection does not necessarily need a deep understanding of the operation of the mind – probabilistic (Bayesian) methods, machine learning and/or data mining approaches applied to regularly collected data can be effectively used to indicate important changes and issues warnings. Our third assumption is that the combination of monitoring (eventually, “measuring”) mental activities with parallel mental training (or “maintenance”) may lead to new scientific observations, and better results (think, for example, on the effects of positive feedback in case of improving performance, or the positive effects of the stress-free, entertaining environment). We also assume that combining mental wellness data with environmental and health data, such as ambient temperature, humidity, atmospheric pressure, blood pressure or level of tiredness, observed at the same time, may give interesting, probably unprecedented results. These assumptions constitute the innovation content of the proposed project.
Our intention is also to organise a virtual multinational mental wellness community where experiences can be exchanged, and our mental wellness toolset can be tested under various circumstances,
The envisaged concept has the following advantages over the state-of-the-art:
- Easy usage: the on-line computer games will be available for everybody who has access to the internet. No installation other than a PC with web access and browser is needed.
- Interesting usage: the mental wellness toolset to be developed will be attractive for elderly people, in popularity similar to word, board and card games, such as Scrabble, Crossword Puzzle, Sudoku, Sharpen-your-mind, etc.
- Combination of mental training and monitoring: this is similar to the combination of physical training and monitoring which is so popular among younger people in these days.
- Active participation: mental wellness training and monitoring assumes active participation of the elderly offering them entertainment and useful pastime occupation at the same time.
- Independent usage: the mental wellness toolset, with on-line computer games, will be designed for individual usage that does not need participation of medical experts. Positive feedback or indications of mental improvements will contribute to the well-being of the given persons; negative indications, on the other hand, should be considered as hints or warnings that a visit to a psychologist, psychiatrist or physician is advisable.
Of course, the approach can also be exploited for other groups of people (e.g. younger people suffering from mental illnesses) and in other countries of the world. As the problem of an aging society is global to all industrialized countries effective solutions for bringing mental wellness training and monitoring to the elderly are demanded worldwide. Therefore, the solutions envisaged in this project have a good chance of being economically successful in many countries. As the system will be developed and produced in European countries, it has a strong European added value, while it can be marketed successfully in almost all industrialized countries.
There are also several questions that need to be answered within this project, among others:
- Is it possible to combine entertaining pastime games with rigorous standard tests?
- Is it possible to measure appropriately the mental and motoric state changes of human beings by interactive games?
- Are the measured data adequate enough to evaluate mental and motoric state changes?
- Is it possible to give medically sound feedback and, if needed, warnings to the user and their relatives or carers in time, based on the described method?
- Is it possible to develop a variety of games that can produce useful measurement data and at the same time satisfy the entertaining needs of a heterogeneous elderly population?
- Is it possible to gain good quantitative results that are useful for the society as a whole?
- Will various elderly groups accept and regularly use such ICT systems? Will such systems meet their expectations?
- Can the planned system be integrated with existing assistance systems?
1.2 Improve quality of life
The earlier one recognises a negative change in his/her own mind or his/her relative’s mental ability the higher the chance is to stop or delay, or at least slow down the speed of any health weakening. Consequently, regular self-monitoring of an elderly person’s mental wellness can extend the time of his/her active and joyful participation in the social life.
As an important result of the project, elderly people will be longer active and keep contact with others in their urban/social environment. Families will also enjoy the mental wellness toolset that could help them to recognise alarming changes in their relatives’ mind. Finally, society will also benefit as elderly will be able to live and stay longer in their homes in an improving (or slower deteriorating) and continuously monitored mental state. The project will bring improvements to the quality of life of the individual, his/her relatives and friends, and thus the quality of life in the whole society will develop.
[...]
Section 2: Project Work Plan
2.1 Concept and methodology
The goals of this project will be reached by setting up a complementary and coherent consortium of eight partners from six partner states (four EU-members and two associated states). Their expertises come from the intersections of broad fields of science, technology, healthcare and social care practise, social responsibilities and business. Works to be done cover studying human behaviour and mental reactions, scientific and medical control of mental state, development of web-based entertaining software, ICT development (e.g. portal, network), and finally, utilization and distribution activities and spreading processes on a profitable and/or non–profitable base.
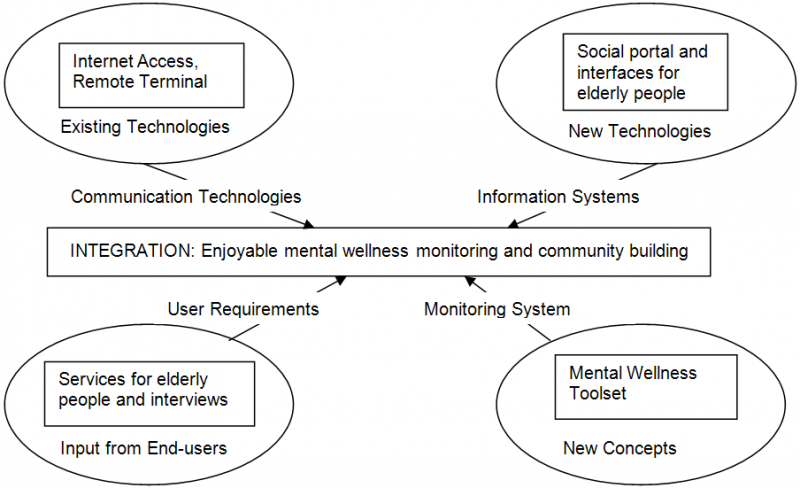
Figure 1: Vision of the M3W project
The project activities can be summarized as follows:
- Survey of needs and opportunities. User, society, healthcare requirements. Complex system requirements.
- System analysis and evaluation. System design. (System in this context means the total conceptual solution as a whole.)
- Analysis and design of technical requirements. Development and – where possible – adaptation of existing knowledge, technologies and solutions.
- Design and development of methodologies for interaction, feedback, consultancies, communication between three functional parties, i.e. elderly end-users, health care background and back-up system.
- Design and building up a Europe-wide data exchange system among back-up suppliers in order to improve quality and also standardise health and elderly services and to solve new challenges due to the increasing elderly population.
- Extension to multinational and multicultural environment. Built up multinational and multilingual communities in order to destroy fences among elderly population in the continent.
- Quality control. System diagnostics, integrity, risk assessment. RAMSS (reliability, availability, maintainability, safety and security) analysis.
- Deployment, evaluation and testing with different kind of end-users (primary, secondary, tertiary).
- Dissemination for different types of end-users (individuals, local communities, etc.) and for different countries.
ICT developments can be summarized as follows:
- Development of specific user-interaction guidelines to fit the needs and abilities of the target population.
- Algorithms for interactive network games.
- Algorithms for measuring and collecting data to be analysed.
- Data analysis individually and data mining statistically.
- Portal development.
- Development of back-up system (including on-line real-time feedback and consultancy).
- Development of a data exchange system.
Dissemination and business activities during the development and the maintenance period can be summarized as follows:
- Selecting and contacting elderly groups (primary end-users) for consultancy and for testing the mental wellness toolset.
- Finding and mobilising elderly groups (living in elderly homes or in their own homes) open to and ready for building a multinational / multilingual / multicultural mental wellness community, and taking part in its activities.
- Finding approaches to reach primary end-users in business-oriented ways.
- Elaborating proper mechanisms and methods to distribute the services of the final system as widely as possible among the elderly.
The initial steps, needed to ensure successful project fulfilment, involve quests in two directions, i.e. the search for appropriate games that can be used interactively and on-line over the network, while deliver measurement data characterising mental wellness state changes; and the search for psychological, mental and motoric parameters that can be reliably measured by these games over long periods of time.
A typical method of experimental neuropsychology is the use of designed experimental tasks, often controlled by computer and typically measuring reaction time and accuracy on a particular task thought to be related to a specific neurocognitive process. An example of this is the Cambridge Neuropsychological Test Automated Battery (CANTAB, http://www.cantab.com) administered to subjects using a touch screen computer. The 22 tests in CANTAB examine various areas of cognitive function, including: general memory and learning, working memory and executive function, visual memory, attention and reaction time (RT), semantic/verbal memory, and decision making and response control. It endeavours to import the accuracy and rigour of computerised psychological testing whilst retaining the wide range of ability measures demanded of a neuropsychological battery. (Popular neuropsychological tests are listed at http://en.wikipedia.org/wiki/Neuropsychological_tests.)

Figure 2: Examples of CANTAB tests: a) Delayed Matching to Sample, b) Graded Naming Test, c) Information Sampling Tasks, d) Big-Little Circle (http://www.cantab.com/science/cantab-tests-all.asp)
For some time, SE PPK and BME EMT have been experimenting with model games seeking for appropriate “devices” to be used in the mental wellness toolset; a few examples are shown below. These simple games, suitable to measure specific neuropsychological parameters, can be developed or combined into more complex, more amusing pastime games.
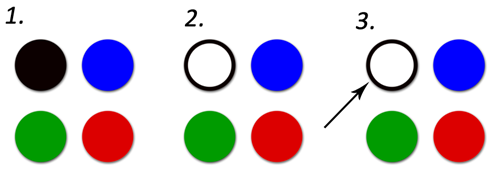
Figure 3. A flashing lights game for measuring changes in mental wellness
Figure 3 illustrates the three phases of the flashing lights game. Phase 1 is the start position, In phase 2, several lights flash in sequence on the screen, and the player has to memorize the order of the flashing lights. Then, in phase 3, the player has to touch the lights in the same sequence.
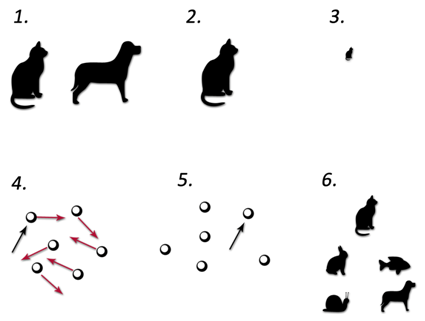
Figure 4. A memory game for measuring changes in mental wellness
Figure 4 illustrates the six phases of another memory game. Phase 1 is a start position where a symbol (e.g. a cat) and its pair (e.g. a dog) are shown. After a few seconds, in phase 2, the pair disappears. Then in phase 3, a few seconds later, the symbol will be displayed in reduced size, surrounded by other figures. In phase 4, all the figures become hidden (e.g. depicted as balls), and slowly shuffled around while the player is expected to follow the movement of the ball that hides the original symbol. In phase 5, the balls stop, and the player is asked to point to the ball containing the original symbol. If s/he succeeds, then in phase 6 s/he is asked to select also the other figure that was in the beginning paired to the original symbol.
At BME EMT and SE PPK, we have made another initial experiment with an interactive game that uses the Wii Remote console of Nintendo. Initially, several (numbered) shapes are displayed and the player is asked to connect them in the order of the numbers by a pen controlled remotely by the Wii console. Thus, not only the mental but also the motoric abilities of the player are tested. The shapes, their amount, placement, size, etc. may be configured, together with several other parameters of the game. The route of the pen is recorded and displayed. We expect that the regular use of the game, and later the analysis of the recorded data may lead to interesting and useful observations of (elderly) players.
Figure 5 shows two snapshots of the game. The left hand side figure shows a situation during the game when the player has already connected the dice #1 and #2, and the pen approaches die #3. The right hand side figure shows a final state, with all dice found, and the full route made by the pen.
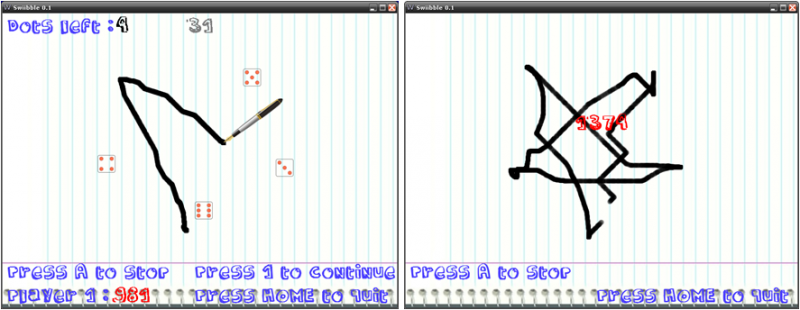
Figure 5. A mental-motoric game for measuring changes in mental wellness
Further, the Israeli company CogniFit has long been involved in the research and development of personalised brain fitness tools (see http://www.cognifit.com), and has the capacity to greatly contribute to the M3W project. CogniFit has significant scientific neuropsychological and medical expertise; its Cognitive Science Department, under the leadership of Dr. Evelyn Shatil, is the scientific basis for age-related research, training and testing activities, and data analysis. In consequence, CogniFit is adding scientific credibility to the project in the field of concept formation, development and validation, which is indispensable for the success of M3W. CogniFit also has years of experience in the field of neuropsychological measurement, data collection, storing and management, and extensive experience and expertise in many computer science domains necessary for the development of neuropsychological computerized activities.
The project concept and achievements will be evaluated during the alpha test phases at the development sites (Hungary, Israel, Luxemburg, Switzerland), and then with end-user partners at pilot sites in Greece and Spain, and at other subcontracted parties in Hungary and Switzerland). It will enable to test the system’s effectiveness and goodness in terms of usability, practicability, reliability and quality (both as measurement tools and as pastime games). On the other hand, the pilot will facilitate close communication with the test participants (elderly persons, nursing home operators and personnel) in order to determine their impressions and wishes needed for extended primary and secondary end-user involvement.
[...]
Section 3: Roles of the consortium partners
3.1 Quality of the Consortium
The consortium consists of seven partners from four countries, including education and research centres (BME EMT, SE PPK, ZHAW), business-oriented SMEs (AI, FZ, Silver) and end-user organisations (FZ, GP).
The members of the consortium have been chosen to fulfil complementary roles. SE PPK brings the psychiatric and psychological expertise into the consortium, and its special experience with mental disorders of the elderly. SE PPK has created the first Hungarian website on neuropsychiatry for the general public (http://www.neuropszichiatria.hu). BME EMT and BME’s cooperating departments have the necessary knowledge and experience in computer science, software development, measurement theory and technology, visualisation, computer graphics, embedded and ambient systems, etc. They are experienced also in R&D project management due to the high number of European and national grants they have won in the past decades. AI and ZHAW have vast expertise in system design, web design, software development, project management and dissemination, and last but not least in exploitation of research results. Silver operates health and welfare oriented portals in Hungary (among others a special one for the 50+), and thus brings business knowledge into the project. The contributions of GP and FZ as small private care companies are extremely important to this project as they represent the secondary end-users in the project, who can reach also a high-number of primary end-users, know well the needs of users, and have hands-on experience about the sustainability of and the business opportunities in care services.
The following paragraphs contain short descriptions of the participating organisations.
AI (Actimage Ltd., http://www.actimage.com) is a European SME established in France, Germany and Luxemburg. Its employees and collaborators are dedicated to consulting, engineering and training in software, multimedia, networks, telecom and security (e-infrastructure), embedded systems, geo-information systems and web engineering. Its core business is focused on web technologies involving the deployment and improvement of standards with regards to accessibility, ergonomics and user experience, interoperability and hosting solutions.
The solid technical and technological background of its taskforce helps Actimage being involved in very ambitious projects, both for large public institutions (cities, counties, regions, ministries and governments) and private key accounts. The company is actually involved in many web projects in which its engineers design user interfaces thanks to well defined user requirements, and contribute to the deployment of ergonomics and accessibility standards. Actimage currently leads an R&D project in the field of diabetes treatment aiming at developing a software assistant for patients to better manage their disease. The software is a mobile application for which Actimage has undertaken the design of innovative interfaces. Actimage has also experience in several national, European and international collaborations. European projects include FP5-IST (EUROPE PKI), Eureka ITEA (ENERGY), Eureka CELTIC (DESYME) and Eureka ITEA2 (GUARANTEE).
The company will share its expertise in, among others, development, interoperability, accessibility and ergonomics standards. Thanks to its involvement in W3C studies, and as part of the ETSI European Consortium, Actimage will mainly be involved in WP4 and WP5, and will actively contribute with up-to-date HMI solutions.
BME (Budapest University of Technology and Economics, http://portal.bme.hu) is the largest school of technology in Hungary, with eight faculties, over 3000 employees and 20 000 students. Its biggest faculty, the Faculty of Electrical Engineering and Informatics (https://www.vik.bme.hu) has ten departments and currently five so called knowledge centres. The latter cooperate closely with the departments and some of the faculties. The Biomedical Engineering Knowledge Centre (EMT) will represent BME in the planned project. EMT is a virtual centre: it executes its R&D activities with the involvement of experts, researchers, PhD and MSc students of various departments of BME, especially with the Dept. of Control Engineering and Information Technology, Dept. of Measurement and Information Systems, Dept. of Telecommunications and Media Informatics, Dept. for Computer Science and Information Theory, Dept. of Psychology and Ergonomics.
BME EMT (BME Biomedical Engineering Knowledge Centre, http://emt.bme.hu) is the technical leader in the running “Silvergate-112: Assistive Medical and Social Monitoring and Alarm System – An Integrated Approach" national project http://silvergate-112.eu), and participates in two currently starting AAL projects (CARE, http://care-all.eu; and CCE), supported by the AAL Joint Programme. The objective of the Silvergate-112 project is to create devices with standardised interfaces and a scalable integration technology that organises devices and services to provide novel services with extended functionality, which would be impossible without integration.
FZ (Frontida Zois Ltd., http://www.frontidazois.gr/index_en.html) is Greece's first private duty home care referral company (SME) providing personal care to help the elderly continue to live independently with the highest level of quality of life that is achievable. Since 2007 when “Frontida Zois” begun operating it has serviced a great number of clients and established an excellent reputation in the Ahaias area, a fact which indicates not only the necessity but also the high quality of the given specialized services. Our caregivers are experienced and qualified professionals providing a variety of services which include hygiene assistance, meal preparation/diet monitoring, light housekeeping, errands and shopping, joyful companionship, etc.
Our company can be of great assistance for the end-users to get familiar to the project considering our experience in association with the elderly people and people with health problems. In a technological project of that range the human presence remains substantial and crucial for obtaining best results. We could describe our contribution as follows:
- To coordinate an End-User Interest Group and make sure that end-users are involved in each step of the solutions design and during lab trials.
- To map and explore the needs of care-recipients and their families and persuade them about the capabilities of the MWT and the beneficiary role that it could play in their lives.
- To enhance through the project development the elderly’s social interaction and motivation.
- To contribute to the elaboration of the results and to suitable correction actions.
- We are in position to evaluate the morphology of each occasion and the possibilities for an individual to be included in such a project.
- We can record any upcoming parameter or particularity from the usage of the system.
GP (Gaudiopolis Retirement Home, http://www.evangelikusbekas.hu) was built by a Lutheran Congregation next to the Lutheran centre: church, parsonage and congregation house. The 64 apartments of the three-storey building of 3600 m² offer comfort and security to the residents. The retirement home is in a garden suburb of Budapest, named Békásmegyer, which is one of the rare districts of the metropolis having the cleanest air. The retirement home operates as a non-profit social welfare institution owned by the parish. Participation in the life of the Lutheran community is not a duty but a possibility, only. Everybody is welcome in the home regardless of his or her religious commitment and denomination.
The foundation-stone of the retirement home funded by donations, own fund, and state subsidy was laid on December 16, 2007, and barely one and a half year later, on June 13, 2009 the congregation, the sponsors and also the new residents (the firsts of whom moved in as early as March 2009) gathered to the official opening ceremony of the retirement home. By opening the home the Lutheran congregation created 50 new jobs besides providing accommodation for nearly 100 seniors.
Each apartment consists of a living room, a non-slip, accessible bathroom and a kitchenette with built-in cupboard and fridge. For the sake of the safety and comfort of the residents each apartment is fitted with nurse-caller, smoke alarm and telecommunication accessibilities, i.e. telephone, cable tv and internet connection. A self-directed lifestyle is offered to the residents in accordance with their age, health condition and demands.
SE (Semmelweis University, http://english.sote.hu), founded in 1769, is the oldest medical school in Hungary. It teaches medicine, dentistry, pharmacy, health sciences, health management as well as physical education and sport sciences. It is named after Ignác Semmelweis (1818-1865), the revolutionary obstetrician who discovered the cause of puerperal fever in the 1840s and therefore is also known as “the savior of mothers”. Today, SE is widely recognized as one of Europe’s leading centers of medicine and health sciences, combining innovation and a time-tested tradition in three main areas: education, research and health care.
SE is a truly international community, embracing over 11,000 students from 60 nations over five continents. Its five faculties offer a wide range of courses from undergraduate to doctorate level in Hungarian, English and German. Foreign students account for about 18% of the total community. SE is the largest health care institution in Hungary with over 9,000 employees covering approximately 6% of the health care needs of the country’s population. With a 238-year-old tradition of academic excellence, SE ranks among the most prestigious Hungarian research institutions where more than 1,300 staff members in approximately 80 departments are involved in R&D activities.
SE PPK (SE Department of Psychiatry and Psychotherapy) is the principal participant in the proposed project (http://www.sote.hu/english/content/info/?inst_id=51). SE PPK houses the Research Laboratory for Neuropsychological Assessment and has a combined experience of over a decade of working with the latest innovations in the field of organic disorders in psychiatry. It has five wards amongst one is exclusively for the treatment of the elderly. It provides the key infrastructural components for the proposed project, including a fully equipped Psychophysiological Laboratory with Electromagnetic (EEG) Tomography and physiological data recording systems (BIOSEMI) as well as a Virtual Environment Development and Testing Unit.
Silver (Silver Kiadó Ltd.) develops and operates the http://otvenentul.hu portal, an online lifestyle magazine targeting people above the age of 50. It is the most well-known medium among portals aiming to reach this age group in Hungary, attracting hundreds of thousands of people each month. The goal of the otvenentul.hu portal is to address questions relevant to the age group above 50; it informs these people in different topics such as health, beauty, financial issues, sports, culture, etc. Reliable and high-quality information is tailor-made to the needs and interests of the target group. Consultants are available on-line to answer specific questions (e.g. questions regarding law, investments, insurance, ailments, psychological issues, solitude, etc.). The portal not only informs but it also entertains and fosters the building of a community. The three main focuses of the portal are health, leisure and community – each of these is fundamental to the quality of life and well-being of the target group. Statistics (March 2009): number of unique visitors: 274 thousand; sex of visitors: 40% men, 60% women; average age of visitors: 55.7 years, place of their living: 37% Budapest (capital), 48% other cities, 15% countryside; level of their education: 44% university or college, 38% high school, 13% skilled workers' school, 5% basic education.
ZHAW (Zurich University of Applied Sciences, http://www.zhaw.ch) is one of the largest and most productive universities of applied sciences in Switzerland, with a strong presence both nationally and internationally. Over 20 institutes and 30 centres at the ZHAW network their resources to provide business and industry with customised services. In 2008, revenues of research funding amounted to 35.5 M CHF and consultancy to 16 M CHF. Three institutes of ZHAW would be connected to co-work with the M3W Project: IFM, IDP and InIT.
The Institute of Facility Management (IFM) is closely involved with partners from business and the public sector, as well as in consulting, research and development, for example: the EU funded MUMMY-project of 4.54 M Euro, concerning Mobile Knowledge Management using multimedia-rich portals for context aware information processing. Since Facility Management has an interdisciplinary character, appropriate combinations of generalists as well as specialists cooperate to solve specific R&D problems. The expertise of IFM can provide any consultancy and research project in conjunction with the adjacent disciplines of Psychology, Service Management, ICT and Knowledge Management and Project Management. IFM has participated in national as well as international (EU-funded) R&D projects.
The Institute of Data Analysis and Process design (IDP) was founded in 2001 and has about 25 employees today with a research budget of about 2 M CHF. IDP is a competence centre for statistical data analysis as well as for modelling and optimization of processes and systems. In the last 9 years, IDP has performed more than 250 projects with companies and public entities, and is heavily involved in national and international R&D projects. Some relevant research directions of IDP are: (1) Business Engineering and Process Management, (2) Technical Systems and Signal Processing, and (3) Data Analysis and Statistics. IDP cooperates closely with the Institute of Applied Information Technology (InIT), which offers a broad spectrum of competencies in the area of information systems and software development. Apart from the technical excellence, InIT also integrates management, legal, human and operational considerations. InIT follows the vision of Smart-IS. The technical leadership is anchored in the four core fields (1) Enterprise-Information Integration, (2) Human-Information Interaction, (3) Information Security and (4) Business-Information Engineering. (Links: http://www.zhaw.ch, http://www.idp.zhaw.ch, http://www.init.zhaw.ch, http://www.ifm.zhaw.ch/nc/en/science/ifm.html).
3.2 User inclusion
The project includes three end-user partners and a special work package (WP2) that deals with the collection and processing of user requirements, to be considered during systems design, as well as with dependability analysis (RAMSS) and dependability requirements. The latter ones include both technical and human factors, taking into account long-term use and deployment under different conditions (e.g., private homes vs. care institutions). The project includes experts as well as carers who are all responsible for the interaction with elderly persons in order to involve them in the system concept elaboration. The project includes SME and institutional partners having healthcare personnel and working directly with end-users, so that they can drive testing and evaluation of the developed system as much as possible in real environments during the whole development process.
3.3 Available resources
All project participants have the required infrastructure for conducting this project. This infrastructure includes psychiatric and technological labs, measuring equipment, instruments and tools for advanced communication in order to work together in an international environment, as well as tools for system and software development and evaluation. Teleconferencing equipment is also available.
Nonetheless, because of the fast obsolescence of computing equipment, each partner plans to buy desktop computers or laptops, and additional computing devices; and eventually software licenses. Such investments are necessary in order to have a harmonised infrastructure at the project partners.
[...]
Section 4: Exploitation of project outcomes
4.1 Demonstration of European wide exploitability
The population trends in the EU27, according to EUROSTAT, clearly show the urging need for technologies supporting the elderly and frail elderly persons, and the potential in the deployment of such assistive systems as the mental wellness toolset (MWT) due to the drastic increase of elderly persons in the coming decades.
Of course, our mental wellness toolset and community approach can also be exploited for other groups of people vertically in the population (e.g. younger people suffering from mental illnesses) and regionally (“horizontally”) in many other countries of the world. As the problem of an aging society is global to all industrialized countries effective solutions for bringing mental wellness training and monitoring to the elderly are demanded worldwide. Therefore, the solutions envisaged in this project have a good chance of being economically successful in many countries. As the system will be developed and produced in European countries, it has a strong European added value and can be marketed successfully in almost all industrialized countries.
Society will benefit as the elderly will be able to live and stay longer in their homes in an improving (or slower deteriorating) and monitored mental state. Families will also enjoy the mental wellness toolset that could help them to recognise alarming changes in their relatives’ mind. The elderly themselves will be longer active and be able to take part in their urban/social environment thereby enriching society.
The targeted system is aimed to be tested in nursing homes, old people’s homes and private home as well because its use assumes only conventional personal computers with internet connection.
Our goal is to reach a penetration of approx. 25% of the elderly population connected somehow to the state sector (dedicated communities, old people’s homes, social institutions, healthcare groups, etc., directed/managed by the state, local governments, civic and church organizations), and approx. 40% of the same population connected somehow to the private sector (profit oriented twilight homes, such homes owned by insurance companies, old people’s day-care centres, care centres and private clinics, etc., and probably above all: the homes of elderly individuals) within 5 years following the development period, i.e. by the year 2018.
4.2 Exploitation capability and time-to-market
Europe is ageing – it is a fact. The forecast for the population trend by 2050 is a clear sign for the high market potential for systems supporting elderly people at home. The targeted system in this project will be developed in collaboration with SMEs having profound experience with ICT-applications for elderly end-users. Furthermore, the project also includes secondary and tertiary end-users who are in contact and provide care for old people directly or who own nursing homes. They will contribute actively to the project ensuring that the planned ICT-system fits well to the needs of elderly people.
With special marketing efforts to our targeted community, primary end-users can be convinced about the advantages of the mental wellness toolset. Marketing can be done by several well-known methods on several well-known media; e.g., through already existing web-sites dedicated to the goal population. Most of these methods, also known as pull methods, makes the client asking directly for the product. These methods will be used here depending on the experiences gained in previous AAL- and other projects of the consortium members.
The best way to win acceptance is to bind opinion-leaders from the psychiatric, medical and care sectors to the project, and to develop the project in cooperation with them in a practical surrounding. This close cooperation is indispensable in order to establish the best possible system on the market and to convince the clients about the product.
After the evaluation of the system and the regional needs, market entrance strategies should be more clearly set-up. This includes the time-intensive exploration of the markets and potential partners as well as choosing adequate, so called distributors/resellers, e.g. portal and web-site service providers, in the different countries and regions. The extension of the partner network is an essential part of the market strategy. Also the adaptation of the product portfolio to the regional particularities has to be facilitated through this strategy.
During the project we shall favour activities which lead to the creation of new patents, which can have a motivating impact on the developers and the business partners.
The system is going to be introduced to the European market within a relatively short period of time. A positive correlation shall be reached in order to lower the subscribing price and the supplying/servicing costs, to increase the numbers and thus to achieve a higher demand for the system. Therefore it will be necessary to include further companies in the distribution cycle. We are going to use experienced marketers who understand how to spread a “product” like this and how to bring suppliers and clients together. For this reason the currently active cooperation with internationally orientated venture capital partners in the web-site business is supposed to have a disseminating role.
No doubt the healthcare sphere as a whole will be a very close and interested partner in our efforts mentioned above.